

INTRODUCTION
Severe fever with thrombocytopenia syndrome (SFTS) is a tick-borne emerging infectious disease caused by a phlebovirus SFTS virus (SFTSV). The major clinical signs and symptoms of SFTS are fever, nausea, vomiting, diarrhea, anorexia, thrombocytopenia, leukocytopenia, lymphadenopathy, and hemorrhagic tendency (1). SFTSV has three segmented genomes composed of large (L), medium (M) and small (S) (2). SFTS was first reported in China in 2011, followed by South Korea, Japan (3, 4, 5). Recently it was also reported in Vietnam and Taiwan (6, 7). Tick is a major vector of SFTSV (8). It has been also suggested that migratory birds might be a carrier of tick bearing from China to South Korea and Japan (9). In South Korea, 1,332 cases had been reported as SFTS including 281 death cases from 2013 to 2020; the case fatality rate was 18.8% (10).
In South Korea, the seroprevalence of SFTS was also known as 2.1–4.1% via ELISA or indirect immunofluorescence assay (11, 12, 13). In China, the seroprevalence of SFTS was also reported as 3.3–9.2% by ELISA (14, 15, 16, 17). In South Korea, the most patients were over than 50 years old and the main occupation of SFTS patients is agriculture and forestry workers (18). In China, agricultural tea pluckers, farming, grass mowing and tick bites were known as risk factors (17, 19, 20). Even more the age is a critical risk factor for severe fever with thrombocytopenia syndrome (14).
Rural areas have been reported as a main outbreak sites of SFTS (11, 18). Island is generally the medically vulnerable area because of geographically isolated by sea and low accessibility to medical resources (21, 22). In addition, it is difficult to know the whole scale of infectious diseases in the medically vulnerable area. Therefore, the rural area of island is also possible to have a high prevalence of SFTS. To the best of our knowledge, seroprevalence of SFTSV antibodies in the medically vulnerable area such as a rural island has not yet been reported. We report a first serosurveillance study of SFTSV antibodies focused on the rural island where were conducted on Mui Island, Incheon, South Korea.
MATERIALS AND METHODS
Ethics statement
The research protocol was reviewed and approved by the Institutional Review Board of Gachon University Gil Medical Center (authorization number: GBIRB2014-314). All participants provided a written informed consent.
Study site
Mui Island, located in Incheon, western South Korea (126.3876–126.4472E, 37.3648–37.4128N; Fig. 1), is a representative rural island of Incheon considering population, occupation, natural environment etc. It has an area of 10.27 km2 and a population of 835 registered persons. The majority of residents are engaged in both agriculture and coastal fishery. The island, which has high colonization of ticks (data not shown), consists of forest 9.27 km2, paddy 0.72 km2, and building site 0.08 km2 and has a temperate climate with four distinct seasons. The average annual temperature is 11.9°C (max 32.0, min -15.9), and the average rainfall is 1186.8 mm.
Recruitment of participants
We recruited a convenience sample in November 2014. In brief, we visited each household in Mui Island and a total of 203 persons (female 127, male 76, 30 to 97 years old, median 67) agreed to participate. The appropriate statistical sample size was supposed as 191. This size was calculated in a descriptive study with a margin of error of 0.05, a confidence level of 95%, and a population ratio of 20%, and population size of 835 (based on the total registered person’s number in Mui Island). A physical examination with a doctor’s interview (eg, fever, gastro-intestinal symptoms) and a standardized questionnaire (eg, age, sex, underlying diseases, history of hospitalization, and occupation) were used whether each participant had symptoms of SFTS or not. Blood samples of 5 mL were collected by venipuncture.
Serological analysis
IgG and IgM against SFTSV in plasma samples were detected separately using indirect immunofluorescence assay with Vero E6 cells infected with SFTSV as described (23). Briefly, SFTSV was isolated from a SFTS patient diagnosed by the Korean Centers for Disease Control and Prevention. Antigen slides of Vero E6 cells infected with SFTSV were prepared. Sera were diluted in 2-fold serial dilutions starting 1:16 to 1:2,048. Sera were placed onto aceton-fixed well slides coated with and reacted at 37°C for 30 min. After incubation, the slides were washed with phosphate-buffered saline. Fluorescein isothiocyanate (FITC)-conjugated anti-human IgG, IgM (Jackson ImmunoResearch Inc, West Grove, PA, USA) was separately added to each well and the slides were incubated at 37°C for 30 min. After washing, the specific fluorescence signals of IgG or IgM against SFTSV were checked by fluorescent microscope (Leica Microsystems, Buffalo Grove, IL, USA). Uninfected cells and normal human serum were used as negative controls, separately. The signals obviously distinctive with negative were accepted as positive. If the signals were on the border with positive and negative, those of next dilution were recognized as positive.
Genetic analysis
For detection of the gene of SFTSV, RNA was isolated from plasma samples using Viral Gene-spin™ Viral DNA/RNA Extraction Kit (iNtRON BIOTECHNOLOGY, Seongnam, South Korea). Nested reverse transcription (RT) PCR was performed for identification of small (S) and medium (M) segment of SFTSV RNA using a DiaStar 2× OneStep RT-PCR Pre-Mix Kit (SolGent, Daejeon, South Korea) with specific primers of SFTSV (Table 1). Both strands of PCR products (346 bp of partial S segment, 360 bp of partial M segment) were cloned and sequenced at least 2 times by TA cloning method using a TOPO TA Cloning Kit (Invitrogen, Carlsbad, CA, USA). Phylogenetic analysis was performed using the neighbor-joining method with the p-distance model in MEGA 6.0. Uukuniemi virus was used as the outgroup.
Table 1.
Primers and annealing temperatures of nested reverse transcription PCR for SFTSV gene
Statistical analysis
Statistical analysis of seropositivity of SFTSV antibodies were performed using Pearson’s Chi-squared test with Yates’ continuity correction or Fisher’s exact test. All statistical analyses were performed using R (version 3.6.3) and R Studio (version 1.3.1093) software. P value only less than 0.05 were accepted statistically significant.
RESULTS
We recruited 203 participants and collected 1 blood sample from each participant with the informed consent in this study. The median age of participants was 67 years old (range from 30 to 97 years). There were 37.4% of male (76) and 62.6% of female (127). All participants were healthy and denied any illness due to SFTSV before involvement of this study.
One participant was positive to both S and M segment of SFTSV via nested RT-PCR. The seroprevalence of SFTSV gene was 0.5% (1/203, 95% CI, 0.01–2.7%). The SFTSV RNA positive participant was a 70-year-old woman with an IgG titer against SFTSV of 1:1,024. To isolate SFTSV from her, we inoculated Vero E6 cells her serum but failed. She was healthy without any symptoms or signs of SFTS, including fever, tick bite rashes etc. Partial sequences of nested RT-PCR products of SFTSV from her serum were deposited in GeneBank (accession no. KR063019–20). The sequences of partial S and M segment showed 94–98%, and 93–97% identity comparing with those of formerly reported SFTSV in Korea, China, and Japan respectively. Phylogenetic trees were also constructed based on both partial S and M segment using the neighbor-joining method (Fig. 2).
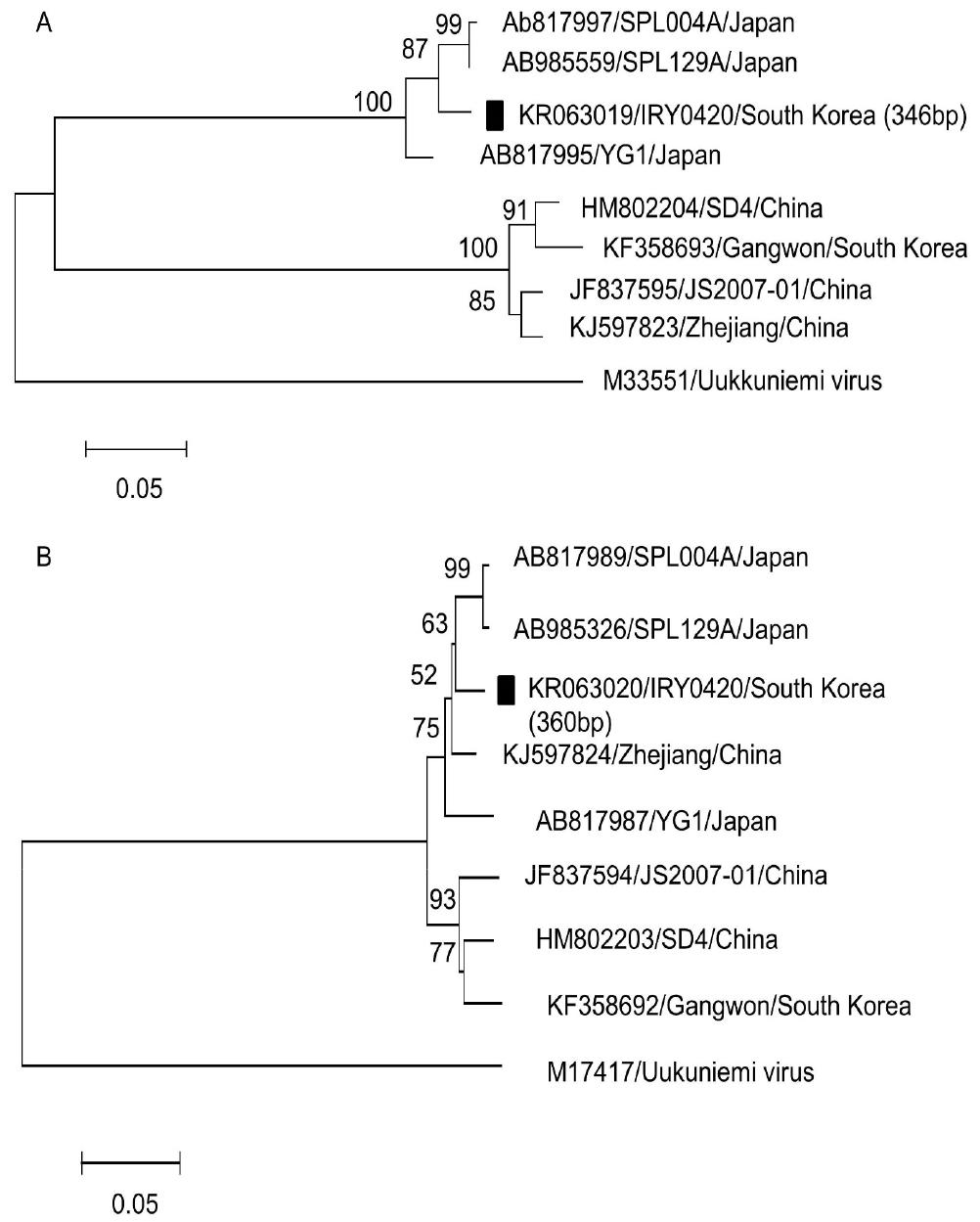
Fig. 2
Phylogenetic analysis of partial segments of severe fever with thrombocytopenia syndrome virus from an asymptomatic participant. The trees were constructed using the neighbor-joining method based on the p-distance model in MEGA6.0 (5,000 bootstrap replicates) based on the partial Small segment (A) and the partial Medium segment sequences (B). Uukuniemi virus was used as the outgroup. GenBank accession numbers precede isolate names and isolated country. Scale bar means 0.05 nucleotide substitutions per sit. The strain isolated on Mui Island is marked with closed square. Numbers at nodes indicate bootstrap values.
Twelve participants (male 6, female 6) were positive to IgG against SFTSV (1:32 to 1:1,024, Table 2) among total 203 participants via the indirect immunofluorescence assay; all including both 1 virus-positive and 12 IgG against SFTSV-positive participants were negative to IgM against SFTSV, a maker of recent infection. Thus, the seroprevalence of SFTSV antibodies in the investigated population was 5.9% (12/203, 95% CI, 3.1–10.1%). The seropositive rate was statically higher in age group >65 than that ≤65 (9.6% vs. 1.1%, OR, 9.202; 95% CI, 1.165–72.692; p=0.026). The seropositive rate of males was 7.9%, which was higher than that of females, 4.7%, but it was not statistically significant. No significant differences in the seropositive rate were also observed according to occupation and duration of residence (Table 3).
Table 2.
Titers of SFTSV antibodies in Mui Island of Incheon, South Korea
| Antibody titer | Seronegative | Seropositive | |||||
|---|---|---|---|---|---|---|---|
| 1:32 | 1:64 | 1:128 | 1:256 | 1:512 | 1:1,024 | ||
| IgG positive (n) | 191 | 3 | 5 | 1 | 1 | 1 | 1 |
Table 3.
Seropositivity of SFTSV antibodies in Mui Island of Incheon, South Korea
| Variable | Participant (n) | IgG positive (n) | Seropositivity (%) | OR (95% CI) | P-value |
|---|---|---|---|---|---|
| Gender | |||||
| Male | 76 | 6 | 7.9 | 1.724 (0.442-6.719) | 0.371 |
| Female | 127 | 6 | 4.7 | ||
| Age, yr | |||||
| ≤65 | 88 | 1 | 1.1 | 9.202 (1.165-72.692) | 0.0262 |
| >65 | 115 | 11 | 9.6 | ||
| Length of residence in Mui Island, yr | |||||
| ≤30 | 85 | 6 | 7.1 | 0.930 | |
| 31 to 60 | 44 | 2 | 4.5 | ||
| >60 | 60 | 4 | 6.7 | ||
| Occupation | |||||
| Agriculture | |||||
| Yes | 119 | 10 | 8.4 | 3.741 (0.767-36.034) | 0.128 |
| No | 84 | 2 | 2.4 | ||
| Coastal fishery | |||||
| Yes | 59 | 6 | 10.2 | 2.590 (0.661-10.161) | 0.111 |
| No | 144 | 6 | 4.2 | ||
| Raising livestock | |||||
| Yes | 4 | 1 | 25.0 | 5.598 (0.099-76.690) | 0.218 |
| No | 199 | 11 | 5.5 | ||
| Business | |||||
| Yes | 35 | 1 | 2.9 | 0.421 (0.009-3.080) | 0.696 |
| No | 168 | 11 | 6.5 |
DISCUSSION
This is the first seroprevalence report of SFTSV in the rural island of Incheon, South Korea. We found the seroprevalence of SFTSV gene 0.5% (1/203, 95% CI, 0.01–2.7%) and SFTSV antibodies 5.9% (12/203, 95% CI, 3.1–10.1%) among the general population on Mui Island, Incheon, South Korea. This study is significant in that it confirmed the seroprevalence of asymptomatic SFTS in the rural island, a medically vulnerable area. So far, no SFTS patients have been reported in Mui Island. This may suggest a lack of proper infectious diseases surveillances and patient reporting in areas with very low access to health care.
In this study, 5.9% of participants in the investigated population were positive for SFTSV IgG although all of them denied any typical symptoms of SFTS. It was suggested that there were also asymptomatic or mild cases of SFTS in central and eastern China (24). This study indicated that subclinical or mild SFTSV infection occurred in the rural island, Incheon, South Korea, as well. Therefore, reported case fatality rates of 18.8% would have been exaggerated because of the subclinical SFTSV infection (3). Case fatality rates of SFTS might be lowered than that supposing clinical and subclinical SFTSV infection cases.
Seroprevalence of IgG against SFTSV among older (>65 years) participants was significantly higher than that of younger (9.6% vs. 1.1%, OR, 9.202; 95% CI, 1.165–72.692; p=0.026). Serological survey from China also indicated that seroprevalence increased with age because exposure to SFTSV may have increased with length of time engaged in outdoor activity (16, 19). The seropositive rate increased significantly with age in southeastern South Korea (11). In this study, it was not statistically different in the seropositive rate according to gender, however, was higher in male than female in Jiangsu, China (19). Moreover, the seropositive rate was not also different according to gender in rural areas of 3 provinces, South Korea (13). This difference might be from the socio-cultural differences among two countries, which the ratio of China male’s outdoor activities in agriculture are higher than that of South Korea’s. The seropositive rate of fruit farmers was also higher than that other farmers in Jeju Island, South Korea (12).
One participant, a 70-year-old female with an IgG titer of 1:1,024 and negative for IgM, was positive to both S and M segment of SFTSV. She denied symptoms of infection. Viremic duration of SFTSV is not well known. According to a study from China, transient viremia preceding seroconversion was suggested because asymptomatic RNA positive blood donors who are negative anti-SFTSV total antibodies were reported (25). In our study, the viremic participant might be in low level viremia after seroconversion because she was positive for IgG. It was also reported that SFTSV had gradually diminished with progression of seroconversion in a naturally infected dog with SFTSV (26).
As some limitations of this study, even though the trained interviewers using the structured questionnaires collected the data about preceding or underlying diseases, tick bite experiences etc, the recall bias could not be completely excluded. Second, since this study was investigated not in all islands of Incheon or South Korea but only a single island of Incheon, however, the external validity might be slightly limited. Third, we evaluated the SFTSV antibody via only indirect immunofluorescence assay not using other methods such as ELISA, neutralization assay etc because of inaccessibility.
In conclusion, we found a seroprevalence of 5.9% in the investigated population. This study suggests that SFTSV readily infects humans in the rural island of Incheon, South Korea; it is necessary to strengthen the infectious diseases surveillance system in rural islands.
